- 501 Orchard Road, #04-08 Wheelock Place, Singapore 238880
- (65) 6235 4429
- hello@vidaskinclinic.com
- (65) 9830 0597
Social media is full of “deep plane facelifts” right now.
The deep plane technique was formally described in 1990 and builds on anatomical work on the SMAS from the 1970s. In other words, it’s not new; it’s a long-standing surgical approach that some surgeons use when appropriate.
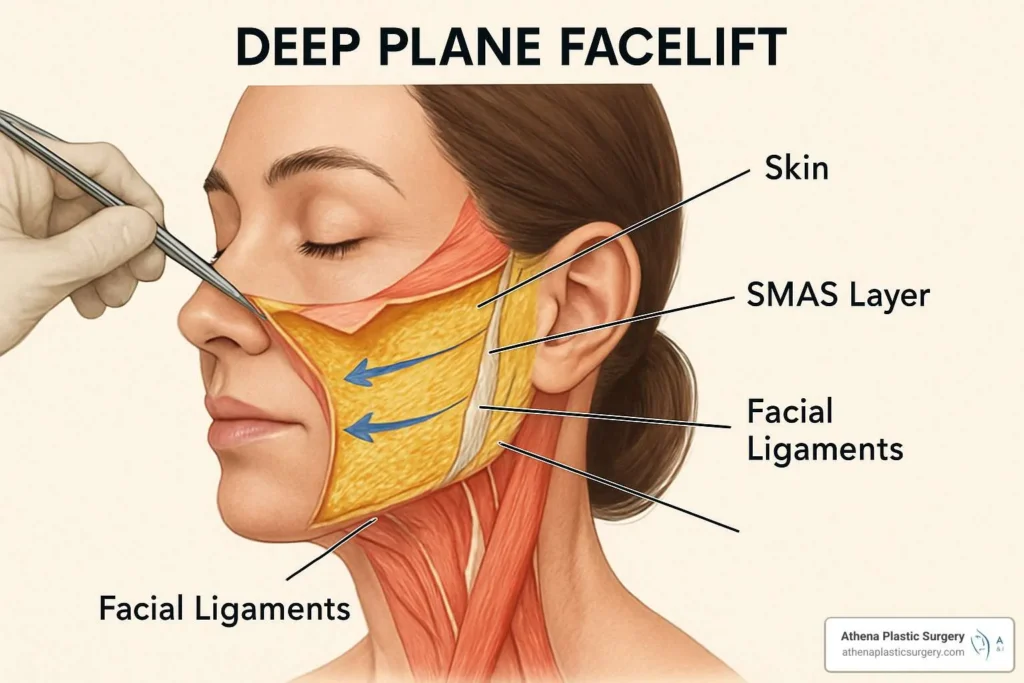
The face is organised in layers: skin → superficial fat → SMAS → deep fat → muscles → bone. The SMAS (superficial musculoaponeurotic system) is the fibromuscular layer surgeons manipulate to reposition descended tissues.

Reality check: “Deep plane” isn’t a brand-new invention; nor is it the only modern facelift method. Surgeons commonly choose among SMAS plication, high-SMAS, deep plane, or combinations, based on anatomy and training. (Technique selection varies; there isn’t a single universal approach.)
A facelift repositions and removes lax skin and re-suspends/supports deeper tissues (e.g., SMAS). It does not reverse intrinsic ageing processes like bone remodelling, fat pad deflation/migration, or long-term skin quality decline. After redraping, excess skin is trimmed; the remaining tissues continue to age with time. (This is why adjuncts such as skin quality treatments or volume restoration may still be considered later.)
All surgery carries risk. Published reviews note the following typical issues discussed during consent:
Neutral note on techniques: Some studies compare complication profiles among SMAS methods (including deep plane and high-SMAS). Differences exist between series, and authors emphasise selecting technique for anatomical goals rather than purely for complication rates.
A facelift repositions lax tissues and removes redundancy; it doesn’t “stop” ageing. Over the years, skin and SMAS can gradually thin and weaken due to biology and time, not because surgery “failed.” This is also why surgical lifting is often combined with skin quality and volume support strategies (before or after) to address other layers.

There is no universally accepted maximum number. Secondary (and tertiary) facelifts are performed, but each subsequent operation is more complex due to altered anatomy, scarring, blood supply, and tissue quality; careful selection and counselling are essential.
For many patients — especially those exploring options before surgery — addressing layers through non surgical facelift treatment rather than “chasing tightness” alone can be prudent:
Our approach: Support each layer appropriately — skin, fat, SMAS/muscle — using evidence-based protocols and conservative dosing, so changes look balanced and remain true to you.
Q1. Is a “deep plane facelift” new?
No. The technique was described in 1990 and builds on SMAS anatomy work from 1976. What’s new is the social media spotlight.
Q2. Is “deep plane” better than other techniques?
Not universally. Surgeons select approaches (SMAS plication, high-SMAS, deep plane, combinations) based on anatomy, goals, and expertise.
Q3. What are the main risks I should know about?
Hematoma, temporary nerve weakness, infection, skin necrosis, and others — with rates varying across studies and patient factors. Discuss personalised risk with your surgeon.
Q4. Does a facelift stop ageing?
No. It repositions tissues and removes redundancy; the face continues to age over time. Skin quality and volume still need consideration.
Q5. Can facelifts be repeated?
Yes, but there’s no fixed limit; secondary procedures are more complex and require careful planning.
