- 501 Orchard Road, #04-08 Wheelock Place, Singapore 238880
- (65) 6235 4429
- hello@vidaskinclinic.com
- (65) 9830 0597

If you have been living with melasma, there is a reasonable chance you have already tried laser treatment — or at least been recommended it. Laser is the most commonly offered treatment for pigmentation in Singapore’s aesthetic industry, and patients with melasma are no exception. The problem is that for melasma specifically, laser is frequently not the most appropriate first-line treatment. In many cases, it exacerbates the condition.
This article addresses the comparison directly: cosmelan and dermamelan versus laser treatment for melasma. It explains the clinical differences, why laser has limitations that are rarely discussed openly, and why a depigmentation programme is the more evidence-based starting point for most melasma patients. If you have been told that laser is the answer for your melasma and the results have been disappointing — or if you are researching your options before committing to any treatment — this article is written for you.
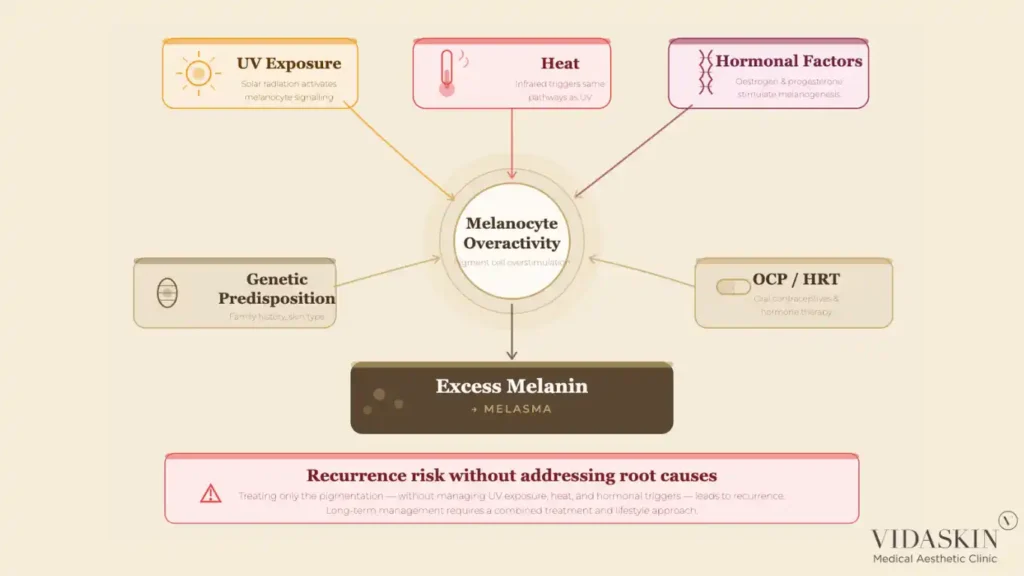
Before comparing treatments, it is essential to understand what makes melasma clinically distinct from other forms of hyperpigmentation. Melasma is not simply a dark spot caused by sun damage. It is a chronic, relapsing pigmentation condition driven by a complex interaction of genetic predisposition, UV exposure, heat, and hormonal factors — particularly oestrogen and progesterone. This is why it is significantly more common in women, and why it frequently appears or worsens during pregnancy, while taking oral contraceptives, or during hormonal shifts.
Melasma presents as diffuse, symmetrical patches of brown or greyish pigmentation — typically on the cheeks, forehead, upper lip, and chin. It affects both the epidermis and, in many patients, the dermis — meaning the pigmentation is distributed across multiple skin layers, not concentrated in a single superficial lesion. This mixed-depth presentation is one of the key reasons melasma is so resistant to treatment and so prone to recurrence.
The defining characteristic of melasma that shapes every treatment decision is this: melasma has ongoing triggers. Unlike a sun spot, which is a fixed lesion that can be targeted and removed, melasma is a condition of overactive melanocytes that continue to overproduce pigment as long as the triggering factors are present. Treating the visible pigmentation without addressing the underlying melanocyte overactivity is the single most common reason melasma treatments — including laser — produce results that do not last.At VIDASKIN, our melasma consultations begin with a thorough assessment of the patient’s hormonal history, sun exposure patterns, skin phototype, and the depth of their pigmentation — because the treatment plan for melasma cannot be determined without understanding these factors.
This point deserves direct and honest treatment because it runs counter to what many patients are told when they walk into an aesthetic practice in Singapore.
Laser treatment is widely recommended for melasma patients across Singapore’s aesthetic industry. Some of these recommendations are genuinely well-intentioned — laser does have a role in melasma management, particularly at low energy settings and as part of a combination protocol. But a significant proportion of laser recommendations for melasma are driven by commercial considerations rather than clinical ones.
Patients presenting with melasma often arrive expecting laser. They have seen it advertised, they associate the technology with modern aesthetic medicine, and they are sometimes sceptical when a doctor proposes something different. Recommending laser to a patient who expects laser is the path of least resistance commercially. It results in a booking, generates revenue from a course of sessions, and satisfies the patient’s initial expectation — at least in the short term.
The clinical problem is that for many melasma patients, laser treatment produces results that are temporary at best and counterproductive at worst. Understanding why requires understanding how melanocytes behave in melasma skin.
Melasma skin contains melanocytes that are chronically sensitised — they are already in a state of heightened reactivity, producing more melanin than normal skin in response to stimuli including UV radiation, heat, hormonal signals, and inflammation. Laser treatment delivers energy to the skin that, even with modern low-thermal technologies, creates a degree of inflammation and thermal stimulation.
In normal skin, this controlled inflammatory response is manageable, and the melanocytes respond predictably. In melasma skin, the sensitised melanocytes can interpret the laser-induced inflammation as a trigger for additional melanin production, resulting in post-inflammatory hyperpigmentation (PIH) that is layered on top of the existing melasma. This rebound effect is well-documented in the clinical literature and is a consistent risk when laser treatment is applied to active melasma without adequate preparation and careful parameter management.
Even when laser does achieve initial lightening of melasma, the improvement is frequently temporary. Because the underlying melanocyte overactivity has not been addressed, the pigmentation returns — often within weeks to months of completing a laser course — as soon as the triggering factors (sun exposure, heat, hormonal fluctuation) resume. Patients who have completed multiple courses of laser for melasma with repeated recurrence are experiencing exactly this pattern.
This does not mean laser has no role in melasma management. At low energy settings, Pico laser toning can be a useful adjunct in a comprehensive melasma programme — but as a supporting measure, not a standalone solution. The distinction matters enormously. Laser, as an adjunct, supervised by a doctor experienced in melasma management, is different from laser as the primary recommendation for a patient who has not yet addressed the root drivers of their condition.

Cosmelan and dermamelan are physician-applied professional depigmentation programmes developed by the Spanish brand Institut Esthederm’s professional division, marketed under the brand name mesoestetic. They are among the most clinically validated and widely used depigmentation systems in the world, with an extensive body of evidence supporting their use in melasma and other forms of hyperpigmentation.
Cosmelan is a multi-active depigmentation treatment that works through a fundamentally different mechanism from laser. Rather than targeting and fragmenting existing melanin, Cosmelan acts directly on the melanogenesis pathway — the biological process by which melanocytes produce melanin in the first place.
The active ingredients in cosmelan — including azelaic acid, kojic acid, phytic acid, ascorbic acid, and arbutin — work synergistically to inhibit tyrosinase, the key enzyme responsible for initiating melanin synthesis. By reducing tyrosinase activity, cosmelan slows and suppresses the overproduction of melanin at its source. This means that rather than removing pigment that has already formed, Cosmelan interrupts the process that keeps creating new pigment.
The treatment consists of a professional in-clinic application of the cosmelan mask — which is left on the skin for a prescribed number of hours before being removed — followed by a home maintenance phase using cosmelan 2 cream, which sustains the depigmentation effect over the months following the in-clinic treatment. The combination of in-clinic intensity and at-home maintenance is what allows Cosmelan to produce durable results in a condition as persistent as melasma.
Dermamelan is the more intensive counterpart to cosmelan within the mesoestetic range, designed for patients with more advanced, deeper, or more resistant melasma. It uses a similar multi-active depigmentation approach but with a more concentrated formulation, producing more pronounced initial results with a correspondingly more intensive post-treatment phase.
Like Cosmelan, dermamelan combines a professional in-clinic mask application with a structured home maintenance programme. The choice between cosmelan and dermamelan — and the specific maintenance protocol — is determined by the treating doctor based on the patient’s melasma severity, skin phototype, and individual response. At VIDASKIN, our doctors assess each patient comprehensively before recommending which programme is appropriate, and provide full guidance on the home maintenance phase that is critical to sustaining results.
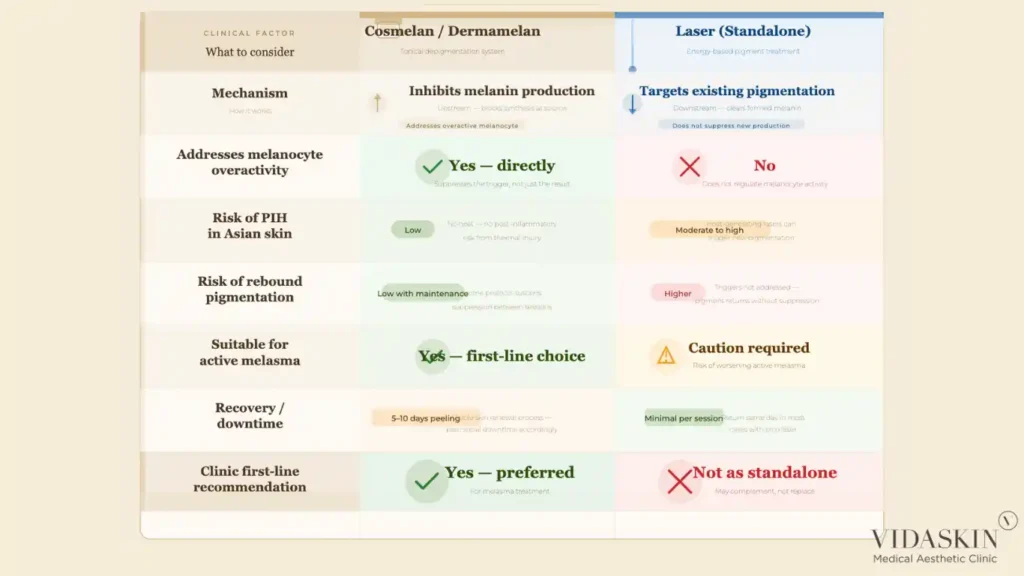
Laser treatment for melasma works by targeting existing melanin — using photoacoustic or photothermal energy to fragment the pigment already present in the skin. It does not inhibit the melanocyte’s ability to produce new melanin. This is the fundamental limitation of laser as a standalone melasma treatment: it addresses the symptom (existing pigmentation) without addressing the cause (ongoing melanocyte overactivity).
Cosmelan and dermamelan work upstream of existing pigmentation — inhibiting tyrosinase and suppressing melanin synthesis at the cellular level. This means the treatment addresses the biological driver of melasma, not just its visible manifestation. Combined with the at-home maintenance phase, which sustains tyrosinase inhibition over time, this approach produces more durable results in a condition characterised by chronic relapse.
Recurrence is the defining clinical challenge of melasma management. Because melasma is driven by ongoing triggers rather than a fixed injury, the pigmentation will return after any treatment — including cosmelan — if the triggering factors are not managed. The question is not whether melasma can be permanently cured, but which treatment approach produces the most durable remission.
The evidence and clinical experience consistently show that treatments targeting the melanogenesis pathway — like cosmelan and dermamelan — produce more sustained remission than treatments targeting only existing pigmentation. Laser treatment achieves visible lightening, but without suppressing melanocyte activity, the melanocytes resume overproduction as soon as the post-laser inflammation resolves and the triggering factors resume. For many patients, this means visible recurrence within two to three months of completing a laser course.
The home maintenance phase of cosmelan and dermamelan is specifically designed to address this recurrence pattern — providing ongoing tyrosinase inhibition that prevents the rapid rebound that characterises poorly managed melasma. Book a melasma consultation at VIDASKIN to discuss which programme is appropriate for your specific presentation and how the maintenance phase is structured.
For Singapore’s predominantly Asian patient population — with Fitzpatrick skin phototypes III to V — the risk of post-inflammatory hyperpigmentation from laser treatment is a genuine and clinically significant concern. Sensitised melasma melanocytes in darker skin phototypes are particularly reactive to the inflammatory stimulus of laser energy, making PIH a common and frustrating complication in patients who undergo aggressive laser treatment for melasma.
Cosmelan and dermamelan carry a different risk profile. The primary post-treatment response is peeling and temporary redness — a keratolytic reaction rather than a thermal one. While the initial post-treatment period can appear intense (the skin undergoes visible peeling over several days), this reaction does not carry the same risk of melanocyte overstimulation as laser-induced inflammation. The risk of treatment-induced PIH is meaningfully lower with cosmelan and dermamelan than with aggressive laser treatment in darker skin phototypes.
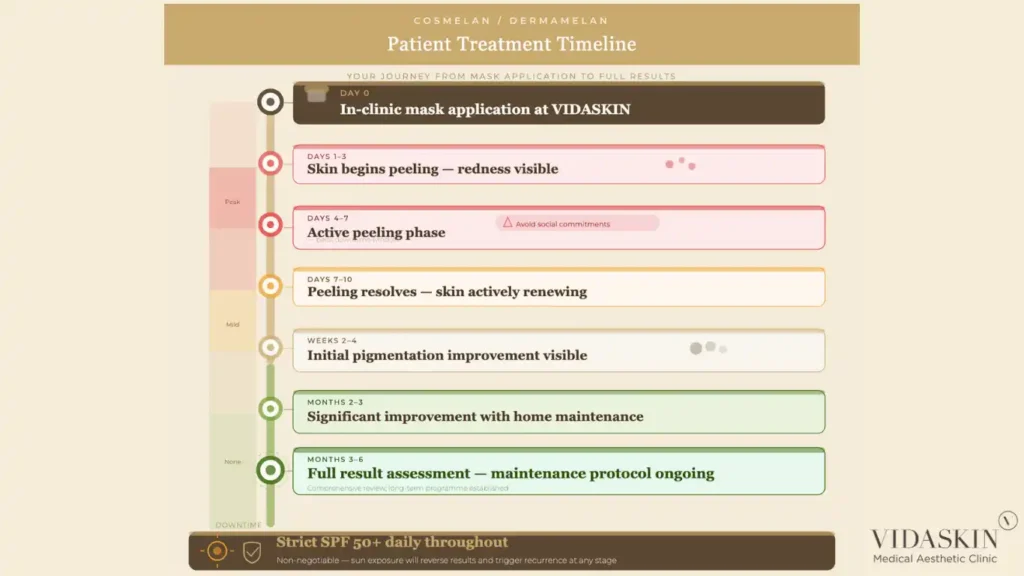
Cosmelan and dermamelan involve a recovery period that patients should be prepared for. In the days following the in-clinic mask application, the skin undergoes visible peeling and redness — a necessary part of the depigmentation process as the surface layers shed and the skin renews. Most patients experience five to ten days of visible recovery, during which social downtime is likely. This is more pronounced than the recovery from a single Pico laser toning session.
However, the relevant comparison is not between one laser session and one cosmelan treatment — it is between a full melasma management programme and a course of laser sessions. When viewed over the same treatment timeline, the total downtime from cosmelan or dermamelan is often comparable to or less than the cumulative downtime from a multi-session laser course — and the clinical outcomes are typically more durable. Our doctors at VIDASKIN prepare every patient thoroughly for the cosmelan or dermamelan recovery process, providing detailed aftercare guidance before the in-clinic application is performed.
Melasma is a chronic condition, and its management should be understood as a long-term commitment rather than a one-time treatment. Both cosmelan/dermamelan and laser require ongoing maintenance — the difference lies in what that maintenance achieves.
Laser maintenance sessions sustain the degree of pigment clearance achieved during active treatment, but without addressing melanocyte overactivity, they are largely reactive — managing recurrence rather than preventing it. Cosmelan and dermamelan maintenance, through ongoing tyrosinase inhibition, actively suppresses the biological process driving recurrence — providing a degree of prevention rather than simply reaction.
In both cases, strict sun protection — daily broad-spectrum SPF 50, reapplied every two hours, with physical sun avoidance during peak hours — is non-negotiable. Without photoprotection, no melasma treatment will produce durable results. Heat avoidance, hormonal management where relevant, and lifestyle modifications are equally important components of a comprehensive melasma programme. Explore the full range of treatments at VIDASKIN and how they are combined to address melasma comprehensively.
In the interest of clinical completeness and honest balance, it is important to acknowledge that laser is not categorically contraindicated in melasma. Its role, however, is specific and conditional.
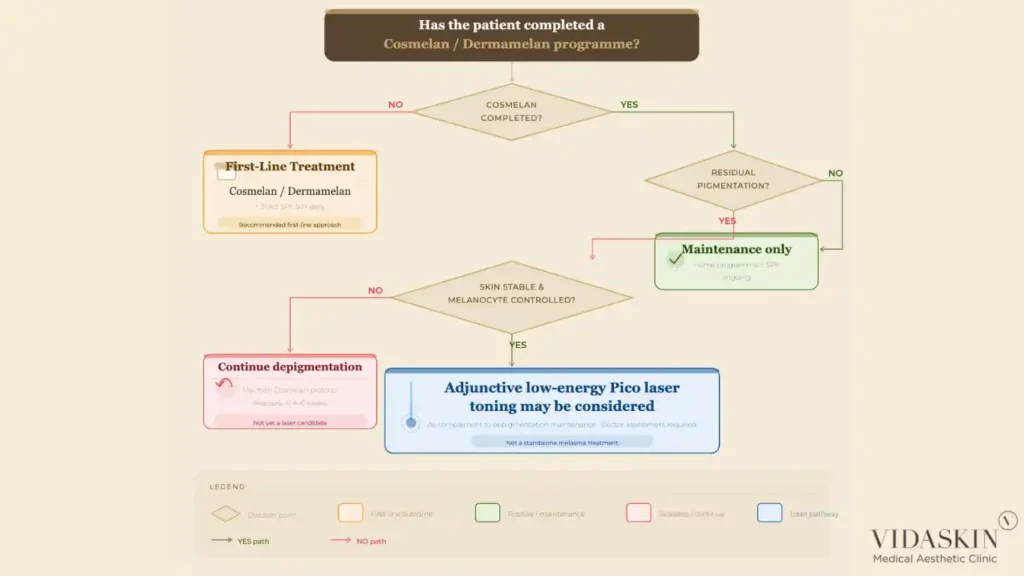
Low-energy Pico laser toning — delivering gentle, sub-ablative energy across the treatment area — can be a useful adjunct in melasma patients who have first completed a course of cosmelan or dermamelan and whose melanocyte activity has been brought under better control. In this context, lasers can help address residual pigmentation that the depigmentation programme has not fully cleared, particularly in cases of mixed epidermal and dermal melasma where the dermal component responds less readily to topical agents.
The key distinction is sequencing and intent. Laser as an adjunct, after appropriate depigmentation, in a patient whose skin has been properly prepared and whose ongoing maintenance is in place — this is a rational clinical approach. Laser as the first and only recommendation for a patient presenting with active melasma, without addressing the underlying melanocyte overactivity — this is where the evidence does not support the practice.
At VIDASKIN, we are transparent about this distinction. If laser has a role in your melasma management, we will recommend it at the right time and in the right context — not because it is the expected recommendation, but because it is the clinically appropriate one.
For most melasma patients, cosmelan or dermamelan is the more clinically appropriate first-line treatment. Laser targets existing pigmentation but does not suppress the melanocyte overactivity driving melasma, which is why recurrence after laser is common. Cosmelan and dermamelan inhibit the melanin production process directly, producing more durable results. Laser may have a role as an adjunct after a depigmentation programme, but it should not be the primary recommendation for active melasma.
Laser is widely recommended for melasma partly because it is what many patients expect, and partly because it is commercially convenient — it generates a course of session bookings and produces visible initial results, even if those results are temporary. The clinical limitations of laser for melasma are well documented but not always communicated honestly to patients. At VIDASKIN, we recommend based on clinical evidence rather than patient expectations.
Initial improvement is typically visible within two to four weeks of the in-clinic mask application, as the peeling phase resolves and the surface pigmentation begins to clear. More significant improvement develops over the following two to three months as the home maintenance phase continues to suppress melanin production. Full results, particularly in deeper or more resistant melasma, are assessed at three to six months post-treatment.
Cosmelan and dermamelan are formulated for use across a range of skin phototypes and are well-suited to the medium-to-dark skin tones common in Singapore’s patient population. The specific programme and maintenance protocol are adjusted based on the individual patient’s skin phototype, melasma severity, and skin sensitivity. A doctor’s assessment is required to determine which programme is appropriate.
Yes. In the days following the in-clinic mask application, most patients experience visible peeling and redness over approximately five to ten days — similar in appearance to a significant chemical peel. Patients should plan for this recovery period and avoid important social or professional commitments during the first week. The downtime is a necessary and predictable part of the depigmentation process.
No. Melasma is a chronic condition with ongoing triggers — including UV exposure, heat, and hormonal factors — that continue to drive melanocyte overactivity. No treatment permanently eliminates melasma. The goal of treatment is sustained remission — reducing the visible pigmentation and suppressing the rate of recurrence through ongoing management. With cosmelan or dermamelan, strict sun protection, and appropriate maintenance, many patients achieve excellent, durable control of their melasma.
Yes — melasma management at VIDASKIN often involves a combination approach. Cosmelan or dermamelan forms the foundation of the programme, supported by strict photoprotection, appropriate topical maintenance, and, where indicated, adjunctive low-energy laser treatment once the skin has been adequately prepared. Your doctor will design a comprehensive programme based on your individual presentation, skin phototype, and treatment history.
Melasma has characteristic features — diffuse, symmetrical distribution on the cheeks, forehead, upper lip, and chin; a tendency to worsen with sun exposure and hormonal changes; and often a mixed epidermal and dermal depth. However, accurate diagnosis requires a doctor’s examination, including dermoscopy where appropriate, to distinguish melasma from other pigmentation conditions such as Hori’s naevus, solar lentigines, or drug-induced pigmentation. Do not begin treatment for pigmentation without a proper clinical diagnosis.
If you have been managing melasma with laser treatment and not achieving the lasting results you were hoping for, you are not alone — and the treatment you have been receiving may not have been the most clinically appropriate choice for your condition.
At VIDASKIN, we approach melasma differently. Our doctors begin every consultation with a thorough clinical assessment — evaluating your pigmentation type and depth, your hormonal history, your skin phototype, and your previous treatment responses — before making any recommendation. If Cosmelan or dermamelan is the most appropriate first step, we will explain why, what the treatment involves, and what realistic results look like. If laser has a role in your programme, we will recommend it at the right time and in the right context.
We are a doctor-owned and doctor-led practice. Our clinical decisions are not influenced by what is easiest to recommend or what generates the most session bookings. We are here to give you an honest assessment and a treatment plan that is genuinely designed to work for your melasma — not one that produces temporary results while the underlying condition continues unaddressed.
We also welcome you to come in and see our before-and-after results from patients treated with Cosmelan and dermamelan. The outcomes speak for themselves.
Book a melasma consultation at VIDASKIN and let our doctors give you a diagnosis-first, evidence-based assessment of your pigmentation — and an honest conversation about which treatment is most likely to make a lasting difference.
