- 501 Orchard Road, #04-08 Wheelock Place, Singapore 238880
- (65) 6235 4429
- hello@vidaskinclinic.com
- (65) 9830 0597

Acne is one of the most common skin conditions presenting in aesthetic and medical clinics across Singapore, and yet it remains one of the most misunderstood. Patients arrive having tried countless products, having read conflicting advice online, and having received different recommendations from different providers. Some have been on antibiotics for years. Others are afraid of isotretinoin despite needing it. Many are spending significant money on skincare that is either inadequate for their condition or actively making it worse.
The truth is that acne treatment is not complicated. When approached systematically, it follows a clear, logical framework that moves from the simplest interventions to the most targeted — and at each level, the clinical rationale is straightforward. The confusion arises not from the complexity of the condition, but from the volume of misinformation surrounding it and the inconsistency of how it is managed across providers.
This article presents acne treatment as it should be understood: a four-tier framework moving from skincare through topical medications, oral medications, and in-clinic treatments — with honest answers to the myths and misconceptions that keep patients from getting the results they deserve.
Effective treatment begins with understanding the condition. Acne is not a hygiene problem, a dietary punishment, or a cosmetic inconvenience. It is a medical condition with a well-understood pathophysiology — and treating it correctly requires addressing its actual drivers, not its surface appearance.
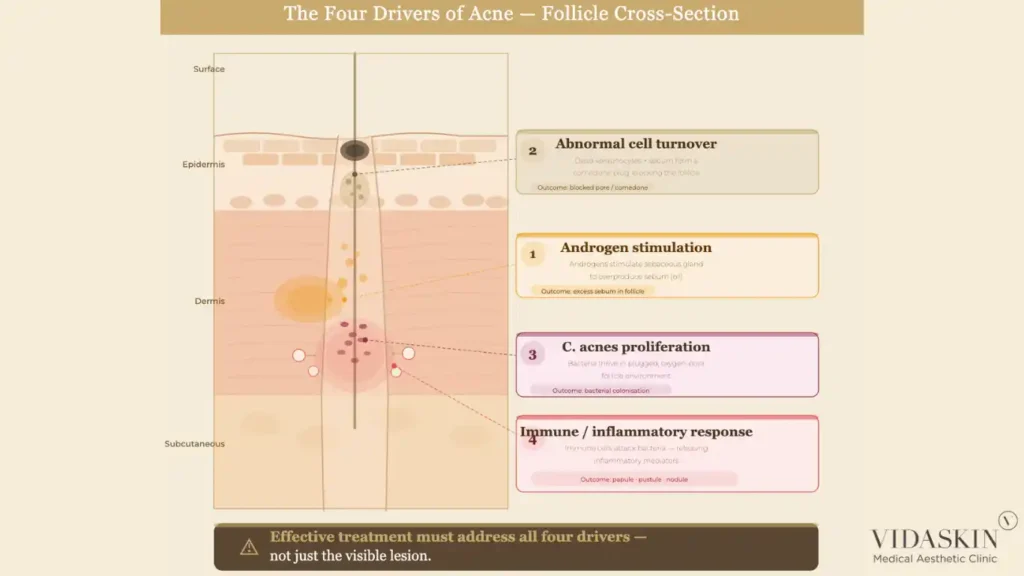
Acne develops through the interaction of four key factors within the pilosebaceous unit — the structure comprising each hair follicle and its associated sebaceous (oil) gland.
Excess sebum production is the starting point. Sebaceous glands, stimulated primarily by androgens, produce sebum that travels up the follicle to the skin surface. When sebum production is excessive, it accumulates within the follicle.
Abnormal cell turnover compounds the problem. In acne-prone skin, the cells lining the follicle shed abnormally, clumping together rather than dispersing. This creates a plug — a microcomedone — that traps sebum within the follicle. This is the origin of blackheads (open comedones) and whiteheads (closed comedones).
Cutibacterium acnes (C. acnes), the bacterium associated with acne, proliferates within the sebum-rich, oxygen-poor environment of the blocked follicle. C. acnes itself does not cause acne — it is a normal skin commensal — but its overgrowth within a plugged follicle triggers an immune response.
Inflammation is the result. The immune system responds to C. acnes activity by mounting an inflammatory reaction within and around the follicle, producing the red, painful papules, pustules, and nodules that characterise inflammatory acne. When this inflammation is severe enough to rupture the follicle wall, it can cause deeper, cystic lesions — and ultimately, the dermal damage that leads to acne scarring.
Understanding these four drivers makes it immediately clear why single-ingredient, single-mechanism treatments rarely resolve acne completely. Effective treatment needs to address sebum regulation, cell turnover normalisation, bacterial load, and inflammation, which is precisely what the four-tier framework achieves when applied correctly.
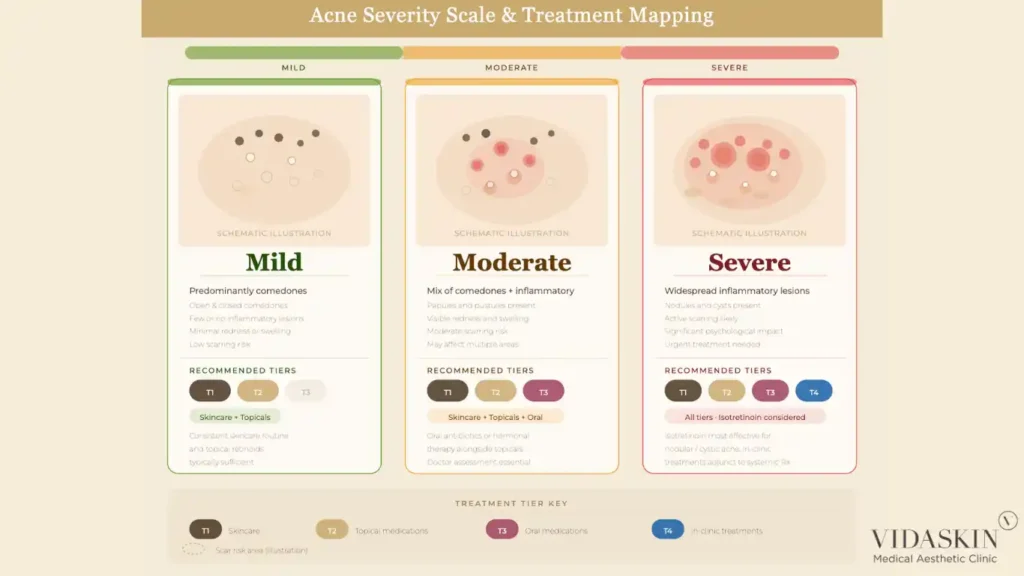
Acne exists on a spectrum from mild comedonal acne — predominantly blackheads and whiteheads with minimal inflammation — to severe nodulocystic acne with widespread deep, painful lesions and significant scarring risk. The severity of a patient’s acne is determined by the relative contribution of each of the four drivers, which varies significantly between individuals.
Patients with predominantly comedonal acne have excess sebum and abnormal cell turnover as their primary drivers — their condition responds well to topical retinoids and appropriate skincare. Patients with moderate to severe inflammatory acne have significant C. acnes involvement and a pronounced immune response — they typically require oral medications in addition to topical treatment. Patients with hormonal acne — characterised by cyclical breakouts around the jawline, chin, and lower face, often in adult women — have androgen-driven sebum excess as a key component, which may respond best to hormonal therapy.
Matching the treatment approach to the individual patient’s acne pattern — rather than applying a generic protocol — is the foundation of effective acne management. This is why a proper clinical assessment is the essential first step before any treatment is recommended.
Hormones are the most significant systemic driver of acne. Androgens — including testosterone and its derivatives — stimulate sebaceous gland activity and are responsible for the surge in acne that commonly occurs during puberty, the premenstrual period, and hormonal shifts associated with contraceptive changes or conditions such as polycystic ovarian syndrome (PCOS). In adult women with hormonally driven acne, addressing the hormonal component — whether through oral contraceptives, spironolactone, or other hormonal agents — is often as important as topical treatment.
Diet has a more modest but clinically recognised role. High-glycaemic foods — those that cause rapid spikes in blood glucose — stimulate insulin and insulin-like growth factor 1 (IGF-1), which in turn stimulate androgen production and sebaceous gland activity. Dairy, particularly skimmed milk, has also been associated with acne in some studies, likely through similar hormonal pathways. These associations are real but individual — not every acne patient will see dramatic improvement from dietary changes, and diet modification should be regarded as a supportive measure rather than a primary treatment.
Stress, sleep deprivation, and certain skincare products (comedogenic formulations) can exacerbate acne in susceptible individuals. A thorough acne consultation at VIDASKIN includes a review of all these contributing factors — because treating acne effectively means understanding the full picture, not just the skin surface.
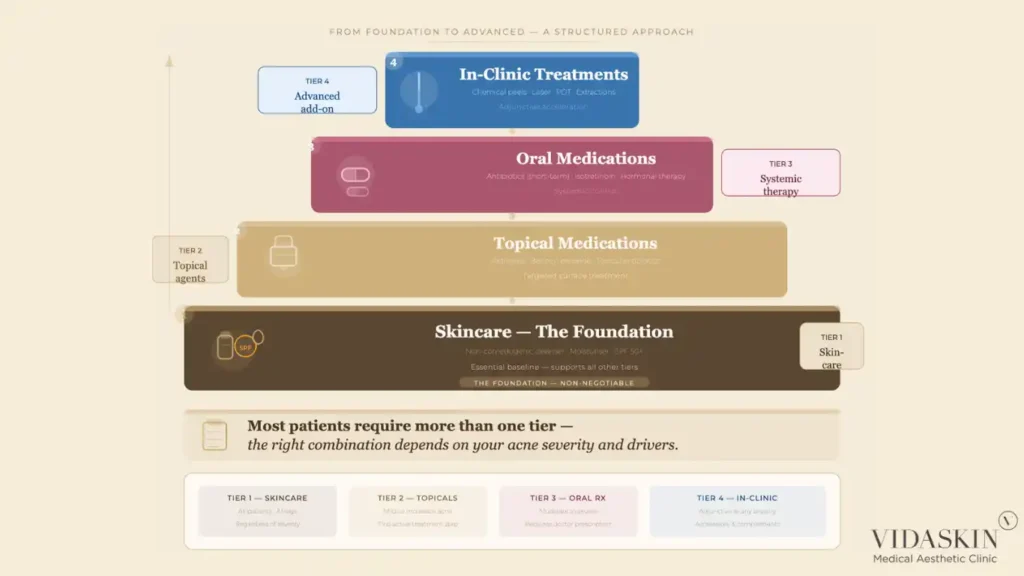
Acne treatment, when approached correctly, follows a logical progression. Each tier addresses acne at a different level of intervention — and in practice, most patients require a combination of tiers rather than a single-tier approach. The framework is simple, and understanding it allows patients to evaluate whether the treatment they have been receiving actually addresses their acne at the right level of intervention.
Skincare is the foundation of any acne management programme. It does not replace medical treatment for moderate to severe acne, but it is an essential prerequisite — the wrong skincare can undermine even the most clinically appropriate medication, while the right skincare supports and amplifies treatment outcomes.
Topical medications are the first line of medical intervention for mild to moderate acne. They act directly at the follicle level — normalising cell turnover, reducing bacterial load, and modulating the local inflammatory response. For many patients with mild acne, topical medications in combination with appropriate skincare are sufficient to achieve good control.
Oral medications provide systemic control of acne drivers that topical treatment cannot adequately reach — including significant C. acnes overgrowth, pronounced sebum excess, and hormonal factors. They are indicated for moderate to severe acne, acne that has not responded adequately to topical treatment, and acne at high risk of scarring.
In-clinic treatments are not a replacement for tiers one through three — they are adjuncts that complement and accelerate the results achieved through appropriate medical management. Patients who seek in-clinic treatments without addressing the medical foundation of their acne are unlikely to achieve lasting results.
The right acne skincare routine is simpler than most patients expect — and considerably simpler than the multi-step regimens often promoted in skincare marketing. For acne-prone skin, the core routine consists of four elements: a gentle, non-comedogenic cleanser; a non-comedogenic, oil-free moisturiser; a broad-spectrum SPF 30 or higher for daytime use; and any prescribed topical medications as directed by the treating doctor.
The cleanser should clean the skin effectively without stripping its natural barrier — a foaming or gel cleanser with a neutral to slightly acidic pH is appropriate for most acne-prone patients. The moisturiser should provide adequate hydration without occluding pores — gel-based or water-based formulations are typically well tolerated. Sunscreen is non-negotiable, both for general photoprotection and because many acne medications increase photosensitivity.
Beyond these four elements, additional skincare products — toners, essences, serums, multi-step treatments — should be evaluated critically for comedogenicity and compatibility with prescribed medications before being incorporated. More is not better in acne skincare; an overcomplicated routine introduces more potential irritants and comedogenic agents than a streamlined one.
Ingredients that support acne management:
Ingredients that commonly worsen acne:
This is one of the most important and counterintuitive points in acne skincare: aggressive cleansing and stripping of the skin does not improve acne — it worsens it. When the skin barrier is repeatedly disrupted by harsh cleansers, alcohol-based toners, or excessive exfoliation, the sebaceous glands respond by increasing sebum production to compensate for the lost lipid barrier. The result is more oil, more pore occlusion, and more acne — the opposite of what the patient intended.
Additionally, a compromised skin barrier allows greater penetration of C. acnes-associated inflammatory mediators into the dermis, amplifying the inflammatory component of acne. Patients who have been cleansing aggressively in an attempt to “clean out” their acne often present with a combination of active acne and a sensitised, reactive skin barrier — which must be restored before more targeted acne treatments can be applied effectively. Our doctors at VIDASKIN review every patient’s current skincare routine at the initial consultation and make specific recommendations to correct approaches that are inadvertently worsening the condition.
Topical retinoids — including tretinoin, adapalene, and tazarotene — are among the most evidence-based medications in acne treatment. They work by normalising follicular cell turnover, preventing the formation of the microcomedones that are the precursor to all acne lesions. By keeping the follicle clear, retinoids address acne at its earliest stage — before sebum accumulates, before C. acnes proliferates, and before inflammation develops.
Retinoids also have a well-documented effect on post-inflammatory hyperpigmentation and on the early stages of scar remodelling, making them doubly valuable in acne patients who also carry pigmentation sequelae from previous breakouts.
The main limitation of topical retinoids is the initial adjustment period — patients commonly experience dryness, peeling, and a temporary flare in acne during the first four to eight weeks of use, as the follicular environment normalises. Patients who are not counselled about this adjustment period frequently discontinue retinoids prematurely, concluding that the treatment is not working or making their skin worse. Proper patient education at the outset is essential to retinoid success.
Benzoyl peroxide is an over-the-counter antimicrobial agent that reduces C. acnes load within the follicle through an oxidative mechanism. Unlike antibiotic-based treatments, benzoyl peroxide does not induce bacterial resistance — making it a clinically important component of acne regimens, both as a standalone agent and as a combination partner with topical or oral antibiotics to prevent resistance development.
Topical antibiotics — most commonly clindamycin — reduce C. acnes activity and have anti-inflammatory properties. They are effective in mild to moderate inflammatory acne but should not be used as monotherapy due to resistance concerns. Combining topical clindamycin with benzoyl peroxide is a standard evidence-based approach that delivers antimicrobial efficacy while minimising the risk of resistance.
For patients with moderate to severe acne — significant inflammatory lesions, nodules, widespread involvement, or rapid scarring progression — topical treatment alone is insufficient. The depth and extent of the inflammatory process in moderate to severe acne exceed what surface-applied medications can adequately address. Attempting to manage significant inflammatory acne with topicals alone delays appropriate treatment, prolongs suffering, and — most importantly — allows scarring to progress that could have been prevented with timely systemic intervention.
Recognising when topical treatment has reached its clinical ceiling and escalating appropriately to oral medications is a key clinical judgement — and one that requires an experienced doctor rather than self-managed skincare. Book an acne consultation at VIDASKIN if your acne has not responded adequately to topical treatment within eight to twelve weeks of consistent use.
Oral antibiotics — most commonly doxycycline and minocycline — reduce C. acnes load systemically and have significant anti-inflammatory properties that make them effective for moderate to severe inflammatory acne. They produce meaningful improvement relatively quickly — often within four to six weeks — and are a valuable short-term tool in the acne treatment armamentarium.
The critical limitation of oral antibiotics is that they are not a long-term solution. Prolonged antibiotic use — beyond three to six months as a standalone treatment — contributes to bacterial resistance, both of C. acnes specifically and of other commensal bacteria more broadly. This is a genuine public health concern, and it is not always communicated clearly to patients who have been on antibiotics for acne for years without a defined endpoint or a plan for transitioning to non-antibiotic maintenance.
The correct role of oral antibiotics in acne treatment is as a bridging therapy — used to rapidly bring inflammatory acne under control while longer-acting treatments (retinoids, isotretinoin, hormonal therapy) are initiated and take effect. They are not intended to be the indefinite, ongoing management strategy for a condition that has a definitive treatment. At VIDASKIN, oral antibiotics are prescribed with a clear endpoint and a transition plan — not as an open-ended repeat prescription.
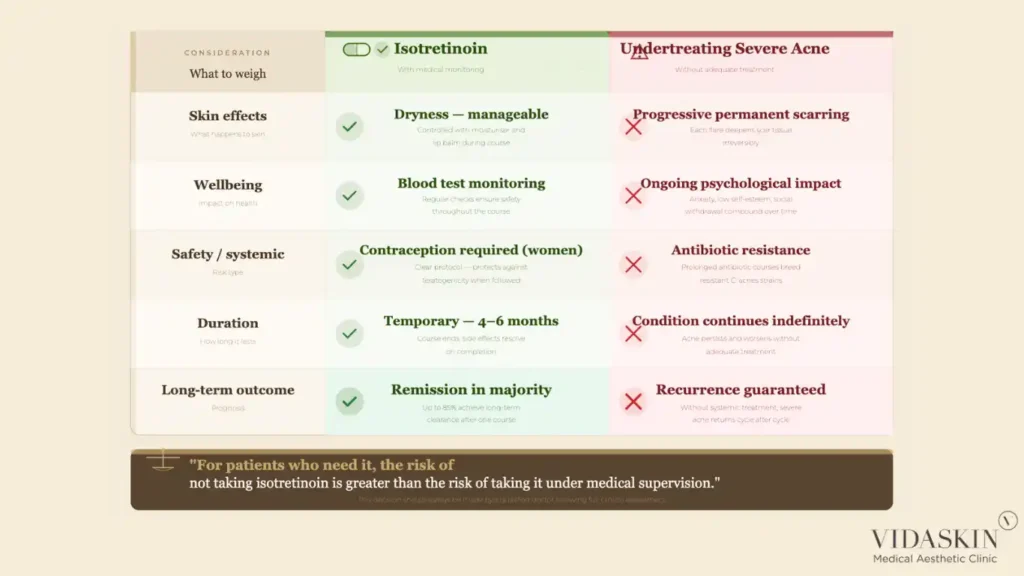
Isotretinoin is, without question, the most effective treatment available for acne. It is the only medication that addresses all four drivers of acne simultaneously — reducing sebum production, normalising follicular cell turnover, reducing C. acnes colonisation, and suppressing inflammation. For patients with severe, nodular, or scarring acne, a completed course of isotretinoin produces long-term remission in the majority of patients — remission that no other treatment can reliably match.
And yet isotretinoin is consistently under-prescribed in Singapore — not because patients do not need it, but because both patients and some prescribing doctors are afraid of it.
The fear of isotretinoin is understandable — it is a potent medication with a well-known side effect profile, and it requires careful management. It is teratogenic and must never be taken during pregnancy, which necessitates reliable contraception in women of childbearing age. It causes dryness of the skin, lips, and mucous membranes in virtually all patients. It can transiently elevate liver enzymes and lipids, which requires monitoring through blood tests during treatment.
What the fear of isotretinoin does not account for is the clinical reality of undertreating severe acne. Every month that severe inflammatory acne goes inadequately treated is another month of potential scarring — scarring that is far more difficult to treat than the acne itself, and that carries a significant long-term psychological and financial cost. The side effects of isotretinoin, when managed by an experienced doctor with appropriate monitoring, are manageable and reversible. The scarring from undertreated severe acne is not.
At VIDASKIN, we have a straightforward clinical position on isotretinoin: for patients who need it, it should be offered. The decision is made through a thorough assessment of the patient’s acne severity, scarring risk, previous treatment history, and personal circumstances — not through fear of a medication whose risks, in context, are well within the bounds of safe, monitored medical treatment. Explore our approach to acne treatment at VIDASKIN and how isotretinoin fits within a comprehensive management plan.
In adult women whose acne has a clear hormonal component — cyclical breakouts around the jawline and chin, acne that worsens premenstrually, or acne associated with polycystic ovarian syndrome (PCOS) — hormonal therapy is a highly effective and often underutilised treatment option.
Combined oral contraceptives containing anti-androgenic progestogens reduce androgenic stimulation of the sebaceous glands, often producing significant improvement in hormonally driven acne. Spironolactone — an aldosterone antagonist with anti-androgenic properties — is another effective option, particularly for women who are not candidates for or who prefer to avoid oral contraceptives.
Hormonal therapy is not appropriate for every patient, and it requires a clinical assessment of the patient’s hormonal history, contraindications, and treatment goals before it is recommended. But for women with clearly hormonally driven acne who have been managed with repeated courses of antibiotics without a lasting resolution, hormonal therapy may be the missing component that finally provides durable control.
Chemical peels — using agents such as salicylic acid, glycolic acid, mandelic acid, or a combination — work by accelerating the shedding of the outermost skin layers and promoting follicular clearance. In acne patients, they are particularly useful for addressing comedonal congestion, reducing the burden of superficial inflammatory lesions, and improving overall skin texture and tone.
Chemical peels are typically performed in a series of sessions spaced two to four weeks apart and are most effective when used as an adjunct to medical treatment, not as a replacement for it. A patient with moderate inflammatory acne who receives chemical peels without appropriate topical or oral medication is receiving an adjunct without a foundation. The peels may improve the appearance of the skin temporarily, but the underlying acne drivers remain unaddressed.
Used correctly — as part of a comprehensive acne programme — chemical peels accelerate the results of medical treatment, reduce post-inflammatory pigmentation, and improve the skin environment in which other treatments work.
Laser and light-based treatments play a supportive role in acne management. Pico laser, in low-energy toning mode, reduces post-inflammatory hyperpigmentation and improves overall skin quality in patients managing active or post-acne skin. Photodynamic therapy (PDT) — which uses a photosensitising agent activated by light to selectively destroy sebaceous glands and reduce C. acnes — has clinical evidence for its use in inflammatory acne, particularly in patients who cannot or prefer not to use systemic medications.
The important caveat — consistent with the approach we apply across all aesthetic treatments at VIDASKIN — is that laser and light therapy are adjuncts, not primary acne treatments. A patient with active moderate-to-severe acne who receives laser treatment without concurrent medical management will not achieve meaningful or lasting control of their condition. In-clinic treatments accelerate and complement medical treatment; they do not replace it.
Manual extraction of comedones — blackheads and whiteheads — by a trained practitioner can provide immediate relief from congestion and improve the appearance of the skin between treatment sessions. When performed correctly, extractions remove the contents of blocked follicles without causing trauma to the surrounding tissue.
The limitations of extractions are that they address existing comedones without preventing new ones from forming — meaning that without concurrent medical treatment addressing the underlying drivers, comedone recurrence is rapid. Extractions are best regarded as a maintenance and comfort measure within a broader acne programme, not a standalone solution.
Patients should never attempt to perform their own extractions at home — aggressive self-extraction is a common cause of post-inflammatory hyperpigmentation, secondary infection, and, in severe cases, acne scarring. If your skin is congested, have extractions performed by a trained practitioner as part of a supervised treatment plan.
The single most important point about in-clinic acne treatments is this: they are most effective when the medical foundation — skincare, topical medications, oral medications where indicated — is already in place. In-clinic treatments are designed to complement a well-managed acne programme, not to replace one.
Patients who attend clinics seeking in-clinic treatments as their primary acne intervention — without appropriate medical treatment — are not receiving the full clinical value available to them. And clinics that offer only in-clinic treatments without properly assessing whether the patient needs medical management are not serving their patients’ best interests.
At VIDASKIN, every acne patient receives a comprehensive assessment that addresses all four tiers. The in-clinic treatments we offer are recommended in the context of a complete programme — not as isolated interventions. Our doctors at VIDASKIN ensure that every patient leaves their consultation with a clear, structured plan that covers all relevant tiers of management.
“Is Acne Caused By Dirty Skin?”
No. Acne is not a hygiene condition. It is driven by sebum excess, abnormal cell turnover, bacterial colonisation, and inflammation — processes that occur within the follicle, not on the skin surface. A patient with acne who washes their face twice daily with an appropriate cleanser is not dirtier than someone without acne. In fact, as discussed above, excessive cleansing in pursuit of a “cleaner” skin actually worsens acne by disrupting the skin barrier and stimulating compensatory sebum production. Acne is a medical condition, not a reflection of personal hygiene.
“Should I Dry Out My Oily Skin?”
No. This is one of the most counterproductive approaches a patient with oily, acne-prone skin can take. Aggressively stripping the skin of oil — through alcohol-based toners, harsh cleansers, or mattifying products that dehydrate the surface — signals to the sebaceous glands that the skin is lipid-depleted, triggering increased sebum production to compensate. The result is more oil, more congestion, and a compromised skin barrier that makes the skin simultaneously oilier and more reactive. The correct approach is to hydrate acne-prone skin with non-comedogenic, lightweight moisturisers — keeping the barrier intact and the sebaceous gland response regulated.
“Are Antibiotics A Long-Term Solution For Acne?”
No, and this is an important conversation that many patients have not had with their prescribing doctors. Oral antibiotics are a valuable short-term tool for bringing inflammatory acne under rapid control. They are not designed — and should not be used — as an indefinite ongoing management strategy. Prolonged antibiotic use without a defined endpoint contributes to antibiotic resistance, disrupts the gut microbiome, and does not address the underlying drivers of acne that will cause it to return once antibiotics are stopped. If you have been on antibiotics for acne for more than three to six months without a clear transition plan, this is a conversation worth having with your doctor.
“Is Isotretinoin Too Dangerous To Take?”
For the vast majority of patients who need it, no. Isotretinoin has a well-known side effect profile that is manageable with appropriate monitoring and patient education. The dryness, the blood test requirements, and the contraception precautions in women are real considerations — but they are manageable ones. What is genuinely dangerous is undertreating severe acne out of unfounded fear of isotretinoin, allowing active inflammation to cause progressive scarring that cannot be reversed. The risk-benefit calculation for isotretinoin in a patient with severe or scarring acne is not close — when properly managed, the benefits vastly outweigh the risks. If you have been told you are “not bad enough” for isotretinoin but your acne continues to scar, seek a second opinion.
“Can Laser Replace Medical Acne Treatment?”
No. Laser and light treatments have a genuine and useful role in the acne treatment toolkit — but they are adjuncts, not primary treatments. They do not address the hormonal, bacteriological, or cell turnover drivers of acne at a systemic or pharmacological level. A patient with active moderate-to-severe acne who receives laser treatment without concurrent medical management may see temporary improvement in skin appearance, but their acne will continue to progress. Laser is most effective — and most appropriately recommended — in the context of a comprehensive acne programme that includes all relevant medical tiers. Clinics that recommend laser as a primary acne treatment without assessing whether the patient needs medication are prioritising in-clinic revenue over clinical outcomes.
“Does Diet Affect Acne?”
Yes — partially. The relationship between diet and acne is real but modest, and it is individual. High-glycaemic diets and, to a lesser extent, high dairy intake — particularly skimmed milk — have the strongest association with acne in the clinical literature, likely through their effects on insulin, IGF-1, and androgen signalling. However, dietary modification alone is rarely sufficient to control moderate to severe acne, and its benefits vary considerably between patients. Diet should be regarded as a supportive measure — worth addressing as part of a comprehensive approach — rather than as a primary treatment or a source of guilt for patients whose acne persists despite dietary changes.

At what age should I see a doctor for acne?
Acne should be assessed by a doctor whenever it is causing distress, leaving marks or scars, or not responding to over-the-counter products after six to eight weeks of consistent use — regardless of age. Adolescent acne that is progressing to scarring, and adult acne that appears for the first time after the age of 25 both warrant early clinical assessment. There is no minimum age threshold for seeking medical management of acne.
How long does acne treatment take to work?
Most topical medications require six to twelve weeks of consistent use before meaningful improvement is visible — patients who discontinue treatment after two to three weeks are not giving it a fair trial. Oral antibiotics typically show improvement within four to six weeks. Isotretinoin produces significant results within the first one to two months of treatment, with a full course typically lasting four to six months. In-clinic treatments such as chemical peels and lasers produce more immediate visible improvements but require a series of sessions for lasting results.
Can acne come back after treatment?
Yes — acne can recur after any treatment, particularly if the underlying drivers are not fully addressed. Isotretinoin produces the most durable remission of any treatment, with many patients experiencing long-term or permanent clearance after a completed course. Patients managed with antibiotics or topical medications without addressing hormonal or lifestyle factors are more likely to experience recurrence when treatment is stopped. Maintenance treatment — typically a topical retinoid — is recommended for most patients to prevent relapse after active acne is controlled.
Is it safe to wear makeup if I have acne?
Yes, provided the products used are non-comedogenic and formulated for acne-prone skin. Mineral-based foundations and oil-free formulations are generally well tolerated. Heavy, oil-based, or comedogenic makeup products can worsen acne by occluding follicles. Always remove makeup thoroughly before applying any topical acne medications, and avoid sleeping in makeup.
Should I pop my pimples?
No. Squeezing or picking at acne lesions disrupts the follicle wall, drives bacteria and inflammatory material deeper into the dermis, and significantly increases the risk of post-inflammatory hyperpigmentation and permanent scarring. If congested skin needs to be cleared, this should be done by a trained practitioner through proper extraction technique — not by the patient at home.
Acne treatment is not complicated — but it does require a systematic, medically grounded approach that addresses the condition at the right level of intervention. The four-tier framework of skincare, topical medications, oral medications, and in-clinic treatments provides a clear roadmap. The challenge is knowing where on that roadmap each patient sits — and ensuring the treatment they receive matches the severity and drivers of their acne, rather than defaulting to whatever is easiest to prescribe or sell.
At VIDASKIN, every acne patient receives a comprehensive clinical assessment — evaluating acne type and severity, scarring risk, hormonal factors, previous treatment history, and current skincare. From this assessment, we design a treatment plan that addresses all relevant tiers, communicates honest expectations about what each treatment can and cannot achieve, and gives patients the information they need to manage their acne for the long term.
As a doctor-owned and doctor-led practice, we do not have a commercial incentive to recommend in-clinic treatments when medical management is what you need, or to keep you on antibiotics indefinitely when isotretinoin is the more appropriate solution. Our recommendations are made on clinical grounds — and we will always tell you what we genuinely believe is most likely to work for your skin.
If you are ready to approach your acne with a clear, structured plan designed around your individual presentation, book a consultation at VIDASKIN. Let us assess your skin properly and give you a programme that actually addresses the condition — not just its surface appearance.
