- 501 Orchard Road, #04-08 Wheelock Place, Singapore 238880
- (65) 6235 4429
- hello@vidaskinclinic.com
- (65) 9830 0597
TLDR: The Identification Guide
Not all scars are the same—and misidentifying your scar type is one of the biggest reasons treatments fail to deliver expected improvement.
While different types of acne leave behind different textural signatures, the healing process generally follows two paths: some scars sit below the skin surface, while others rise above it. In some cases, the marks left behind aren’t permanent scars at all.
This guide breaks down the two major scar categories, explains common look-alikes, and shows how various types of acne evolve into permanent “legacy” scarring—so you can understand what you’re actually dealing with before considering treatment.
Before classifying scars, it’s important to rule out one common confusion.
Post-Inflammatory Erythema (PIE) appears as:
PIE is not a scar. It represents vascular damage, not collagen loss.
Because PIE involves dilated or damaged blood vessels, it responds better to vascular-targeting lasers (such as VBeam) — not resurfacing or scar-release treatments used for pitted scars.
If the skin looks red but feels smooth, you’re likely dealing with PIE rather than true scarring.

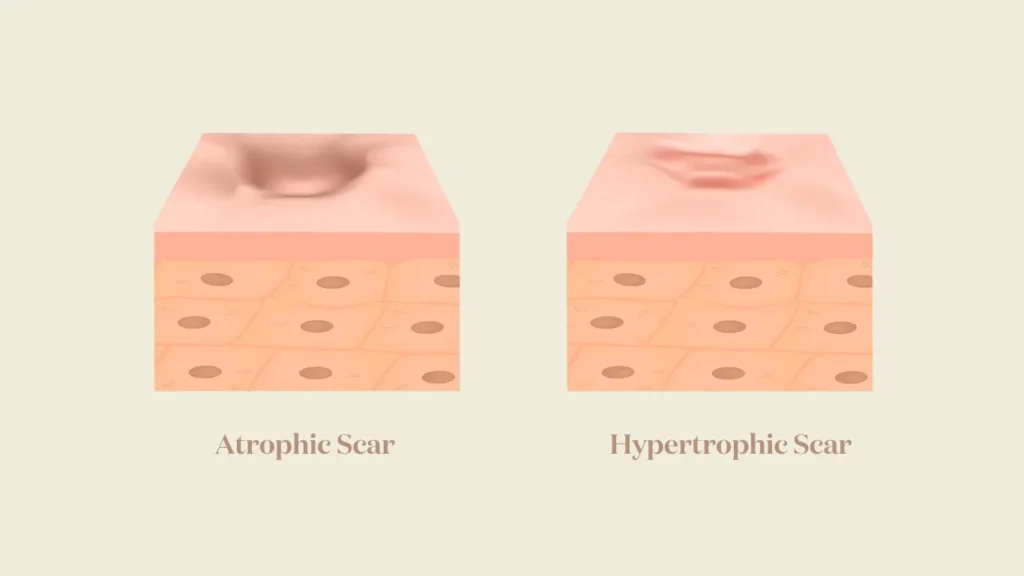
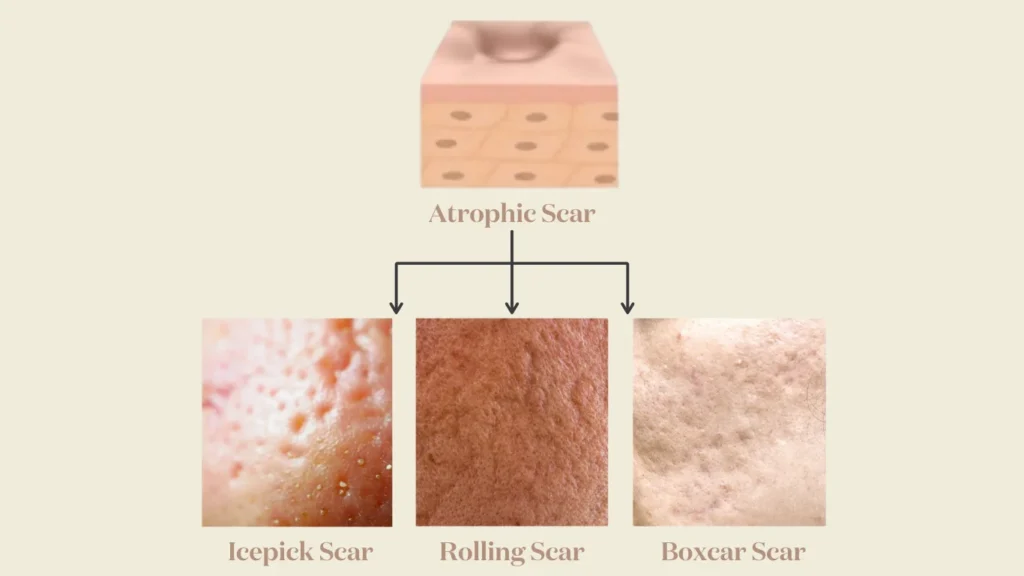
Atrophic scars are depressed scars that result from insufficient collagen production during the healing process. They sit below the surrounding skin surface.
Most atrophic scars fall into what’s known as the Atrophic Trinity — the “Big Three”:
These are often the most challenging to treat due to their depth and narrow shape.
They often respond well to resurfacing when not deeply tethered.
Rolling scars are commonly tethered, which affects treatment planning.
A simple self-assessment called the ‘Pinch Test’ can help identify scar depth.
How to do it:
What it tells you:
Tethered scars often require mechanical release (subcision) before resurfacing can be effective.
Raised scars result from excess collagen production, not loss.
This distinction matters because hypertrophic vs. keloids behave very differently and require different management approaches.

Scar behaviour isn’t random.
Genetic predisposition plays a major role in how skin heals:
Skin type, ethnicity, family history, and inflammatory response all influence which direction healing takes.
This is why identical acne severity can leave very different scarring patterns in different people.
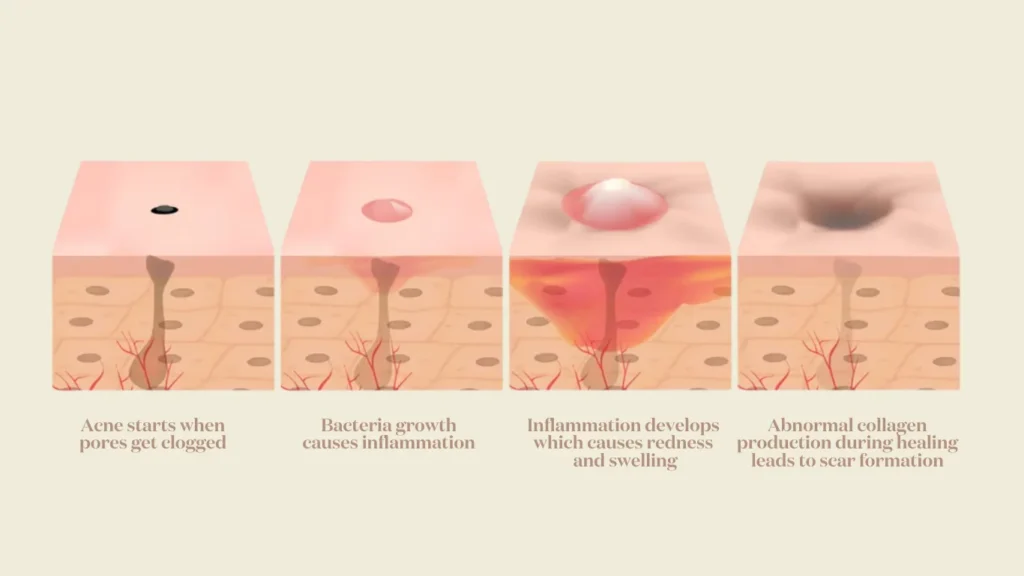
Scars don’t appear overnight.
The transition from active acne to “legacy” scarring happens quietly — and reminds us there is a critical window for early intervention.
Treating inflammation early reduces the risk of collagen damage that leads to permanent scars.
Atrophic scars, hypertrophic scars, keloids, and PIE may coexist on the same face, but they are not treated the same way.
Correct identification helps determine:
Understanding your scar type is not about labels. It’s about choosing approaches that work with your skin biology instead of against it.
While this guide provides the tools for self-assessment, it is common to find that your skin displays a combination of these textures simultaneously. Navigating the various types of acne scars can feel overwhelming, but pinpointing whether your skin is losing collagen (atrophic) or producing too much (hypertrophic) is the essential first step.
By accurately categorizing the types of acne scars present on your skin, you can have a much more productive conversation with a dermatologist and build a treatment roadmap that addresses your specific skin history with precision.
If scars are the result of how your skin healed in the past, then identifying them correctly is how you shape its response going forward.
Once you can tell what kind of scar you have, you’re no longer guessing — you’re planning.
