- 501 Orchard Road, #04-08 Wheelock Place, Singapore 238880
- (65) 6235 4429
- hello@vidaskinclinic.com
- (65) 9830 0597

Hyperpigmentation is one of the most common skin concerns among patients in Singapore — and one of the most misunderstood. The term covers a wide range of conditions, from straightforward sun spots to complex, hormonally driven melasma, and not all of them respond to the same treatment. Pico laser has become a widely used tool for pigmentation management, but its effectiveness and appropriateness depend entirely on what type of pigmentation is being treated and whether the diagnosis has been made correctly.
This article explains how Pico laser targets melanin, why it is considered safer for darker skin types, what realistic results look like and when, and — critically — why a proper medical diagnosis before any treatment is not optional. It also addresses a topic that is rarely discussed openly in Singapore’s aesthetic industry: why laser treatment is frequently recommended for melasma patients when it should not be the first choice.
Melanin is the pigment produced by melanocyte cells in the skin, and it is the primary chromophore — the light-absorbing target — for most pigmentation laser treatments. Understanding how Pico laser interacts with melanin explains both its effectiveness and its safety advantages over older laser technologies.
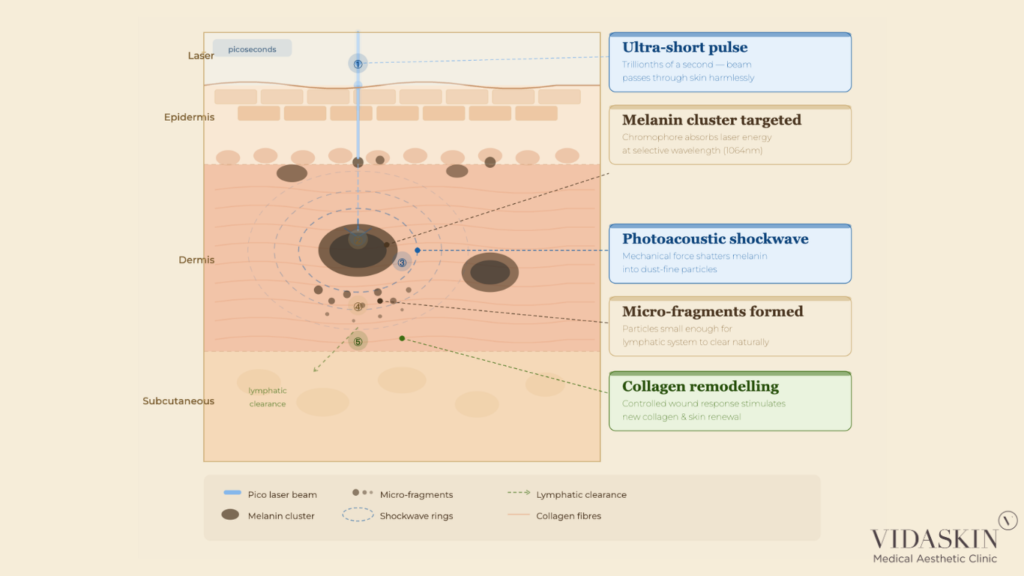
When a Pico laser pulse is directed at a pigmented lesion, the energy is selectively absorbed by the melanin within the target cells. The key distinction of the Pico laser is not the wavelength — it is the pulse duration. At picosecond speeds (trillionths of a second), the energy is deposited into the melanin so rapidly that it creates a photoacoustic shockwave rather than a thermal reaction.
This shockwave physically fractures the melanin cluster into extraordinarily fine, dust-like particles — significantly smaller than the fragments produced by nanosecond laser systems. The importance of this cannot be overstated: the finer the fragmentation, the more efficiently the body’s immune system can identify, engulf, and clear the particles through the lymphatic system. What takes the body weeks to clear with coarser nanosecond fragmentation may be cleared in a shorter timeframe with the finer particles produced by Pico energy.
This is why, when performed correctly on the right type of pigmentation, Pico laser can produce more complete clearance with fewer sessions than traditional laser systems — not because it uses more power, but because it produces a more physiologically manageable fragment size. At VIDASKIN, our doctors use Pico laser selectively — only for pigmentation types where it is clinically indicated — rather than as a default recommendation for any patient presenting with a dark spot.
Following a Pico laser session, the fragmented melanin particles do not disappear immediately. The process of clearance is biological — it depends on the activity of macrophages and the lymphatic system, which are responsible for removing cellular debris and foreign particles from the tissue.
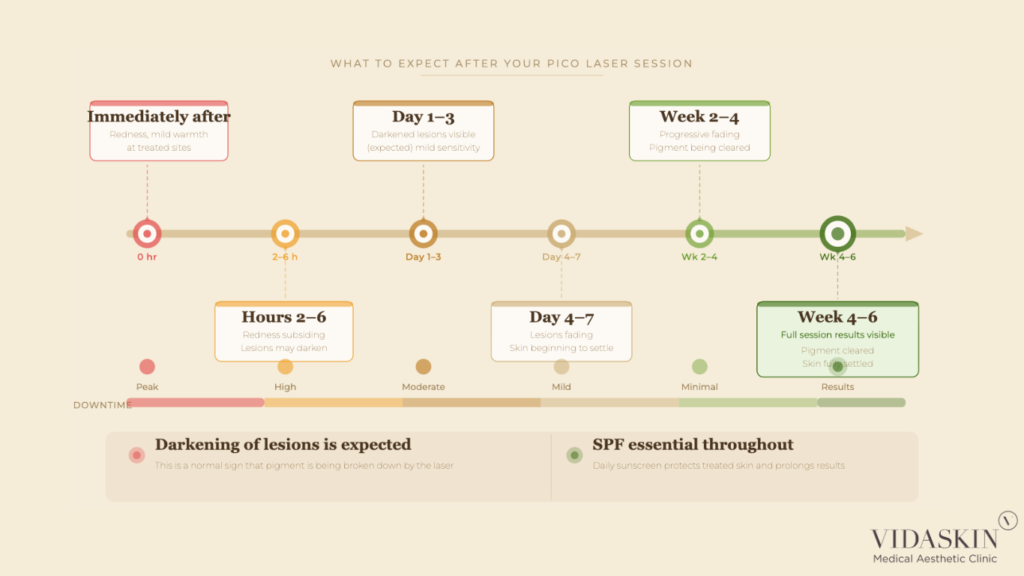
This natural clearance process is gradual and cumulative. In the days immediately following treatment, the treated lesion may appear darker — this is because the fragmented pigment is still present within the tissue, but the surrounding skin has been temporarily disrupted. Over the following two to four weeks, as macrophages engulf and transport the particles away, the lesion progressively lightens.
This timeline varies between patients based on immune system efficiency, skin phototype, the depth of the pigmentation, and how diligently post-treatment sun protection is maintained. Patients who expose treated skin to UV radiation during the clearance phase risk stimulating new melanin production in the disrupted tissue — potentially darkening the lesion again and undoing the progress made by the laser session.
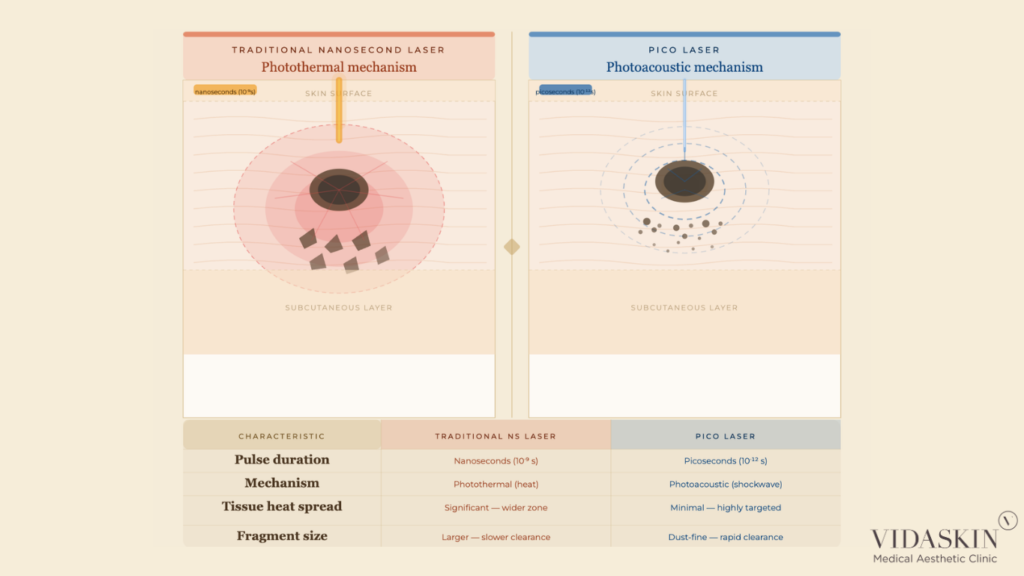
The clinical differences between Pico laser and traditional nanosecond Q-switched laser treatments are most apparent in three areas: fragment size, thermal risk, and suitability for darker skin phototypes.
Traditional nanosecond lasers also target melanin selectively, but the longer pulse duration means more energy is converted to heat before the pulse ends. This heat spreads to the surrounding tissue — a phenomenon known as thermal diffusion — and creates a risk of collateral damage to the dermis and adjacent melanocytes. In darker skin types, this thermal injury can paradoxically stimulate the very melanin production it is intended to reduce, resulting in post-inflammatory hyperpigmentation (PIH) that is often worse than the original lesion.
Pico laser’s ultra-short pulse duration minimises thermal diffusion, reducing the risk of collateral thermal damage. The photoacoustic mechanism achieves comparable or superior pigment fragmentation at a lower thermal load, which is the fundamental reason it has become the preferred technology for pigmentation treatment in Asian skin. Learn more about how our doctors at VIDASKIN approach pigmentation diagnosis and laser selection for each patient.
Singapore’s patient population spans a wide range of skin phototypes — predominantly Fitzpatrick types III to V — for whom the risk of laser-induced PIH is a genuine and significant clinical concern. The safety of any laser treatment in this demographic is not simply a matter of technology; it is a matter of correct diagnosis, parameter selection, and clinical experience.
PIH is a darkening of the skin that occurs in response to inflammation or injury, including the controlled injury created by laser treatment. In darker skin phototypes, melanocytes are more reactive and more easily triggered by thermal stimuli, making them particularly susceptible to PIH following photothermal laser procedures.
Because Pico laser generates significantly less heat in the surrounding tissue than nanosecond lasers, it produces a milder inflammatory response — and consequently, a lower risk of PIH. This is not a categorical guarantee: PIH can still occur with Pico laser if energy settings are inappropriate for the patient’s skin phototype, if the skin is inflamed or compromised at the time of treatment, or if post-treatment sun protection is inadequate. However, when performed correctly, the risk is meaningfully lower than with traditional photothermal laser systems.
This reduced PIH risk is particularly relevant for patients with skin phototypes IV and V — common in Singapore’s Chinese, Malay, and Indian patient populations — for whom aggressive photothermal laser treatment carries a considerably higher complication risk.
Asian skin presents specific characteristics that influence laser treatment outcomes. Compared to lighter phototypes, Asian skin tends to have more reactive melanocytes, a higher baseline melanin concentration, and a greater tendency to respond to inflammation with pigmentation changes rather than redness. These characteristics make it simultaneously more prone to PIH and more in need of precise, low-thermal-load treatment approaches.
Pico laser addresses these characteristics more effectively than most alternatives currently available. Its photoacoustic mechanism, reduced thermal diffusion, and ability to fragment melanin into finer particles that clear more efficiently make it one of the most appropriate laser technologies for the range of pigmentation conditions commonly presenting in Asian skin — including solar lentigines, post-inflammatory hyperpigmentation, and certain types of dermal pigmentation such as Hori’s naevus.
That said, “Pico laser is safe for Asian skin” is not a blanket endorsement of Pico laser for all pigmentation in all Asian patients. The specific condition, its depth, and the patient’s individual skin reactivity all determine whether Pico laser is appropriate — and at what parameters. This is why a doctor’s assessment is not a formality; it is the foundation of safe treatment. Book a pigmentation assessment at VIDASKIN to have your skin evaluated by a doctor before any laser treatment is scheduled.
Beyond PIH, other potential side effects of Pico laser in darker skin types include transient hypopigmentation (lightening of the treated area), rebound pigmentation if treatment is too aggressive, and — in rare cases — textural changes if energy settings are excessive for the skin’s tolerance.
These risks are minimised through correct patient selection, conservative parameter choices, adequate treatment intervals to allow full recovery between sessions, and strict post-treatment sun protection. A doctor who is experienced in treating Asian skin will start conservatively, assess the skin’s response after each session, and adjust parameters progressively — rather than applying a fixed, high-energy protocol from the outset in the interest of faster results.

One of the most important aspects of managing patient expectations around Pico laser for hyperpigmentation is the timeline of results. Patients who expect to see cleared skin immediately after a session will be disappointed — and may incorrectly conclude that the treatment has not worked.
The temporary darkening of a treated pigmentation lesion following Pico laser is not a sign of failure or adverse reaction. It is a predictable and expected part of the treatment response, and patients should be counselled about it before their first session.
The darkening occurs because the fragmented melanin particles are still present within the tissue in the days immediately following treatment — they have been broken down but not yet cleared. The disruption to the surrounding skin caused by the laser can make the lesion appear more prominent before the clearance process begins in earnest. In some cases, the treated area may develop a greyish or brownish crust, particularly with higher-energy settings, which naturally sloughs off as the skin heals.
Understanding this progression — darkening followed by gradual fading — prevents patients from panicking in the first week post-treatment and, critically, from taking interventions (such as scrubbing or picking at the treated area) that could interrupt the healing process and increase the risk of PIH or scarring.
As a general guide, the following timeline applies to most epidermal pigmentation treatments with Pico laser:
Dermal pigmentation — such as Hori’s naevus or deep melasma — clears more slowly than epidermal pigmentation, as the fragmented particles must travel from a deeper tissue layer to reach the lymphatic system. Patients with dermal involvement should be counselled for a longer overall treatment timeline and more gradual per-session improvement.
Monitoring is an active clinical process, not a passive wait. At each follow-up visit, the treating doctor should assess how the skin has responded to the previous session — evaluating the degree of pigment clearance, any signs of PIH or other side effects, and the current condition of the skin — before determining the parameters for the next session.
This session-by-session assessment allows the protocol to be refined as the treatment progresses. A patient whose skin responds strongly to a conservative initial session may be able to tolerate slightly higher energy in subsequent sessions; a patient who shows early signs of PIH requires a longer interval and lower energy to allow the inflammatory response to fully resolve before retreating. Our doctors at VIDASKIN conduct a clinical skin review at every visit — treatment decisions are never made on autopilot or according to a fixed schedule, regardless of how the skin is responding.
This is the section of the article that matters most — and the one that is most often glossed over in aesthetic marketing content. Before any pigmentation treatment is recommended, the nature of the pigmentation must be correctly diagnosed. Not all dark spots are the same, and not all of them should be treated with a laser.
The vast majority of pigmented lesions presenting in an aesthetic practice are benign — solar lentigines, seborrhoeic keratoses, post-inflammatory hyperpigmentation, and freckles are common examples. These are cosmetic concerns and appropriate candidates for aesthetic treatment, including Pico laser, where indicated.
However, some pigmented lesions require a very different response. Melanoma — the most serious form of skin cancer — can present as an irregular, darkened lesion that may superficially resemble a benign pigmented spot. Other conditions, including pigmented basal cell carcinoma and dysplastic naevi, also require medical evaluation before any laser or aesthetic treatment is considered.
Treating a malignant or pre-malignant lesion with laser energy is not merely ineffective — it is potentially dangerous. Laser treatment of a melanoma does not remove or destroy the cancer; it disrupts the lesion’s appearance in a way that may delay diagnosis and allow the malignancy to progress. A doctor who examines a lesion properly — using dermoscopy where indicated — before recommending treatment is performing an essential clinical service, not simply a procedural step.
This is why pigmentation treatment should always begin with a proper medical consultation, conducted by a licensed doctor who is trained to distinguish cosmetic concerns from conditions requiring medical intervention. It is not a bureaucratic requirement — it is patient safety.
Certain pigmentation presentations warrant referral or further investigation before any aesthetic treatment is initiated. These include asymmetrical lesions, have irregular borders, show variation in colour within the lesion, have a diameter greater than 6mm, or have changed in size, shape, or colour over a short period — collectively referred to as the ABCDE criteria for melanoma evaluation.
Other presentations that require medical evaluation before laser treatment include any lesion that bleeds spontaneously, any new lesion appearing rapidly in an adult, or any pigmented lesion in an immunocompromised patient. In these cases, the appropriate first step is a medical assessment — and potentially a referral to a dermatologist or oncologist — before any cosmetic intervention is considered.
A competent aesthetic doctor will recognise these presentations and act accordingly, even when the patient’s primary desire is cosmetic treatment. This is an area where the doctor-owned, doctor-led model of care matters enormously — a commercially driven practice has an incentive to proceed to treatment; a doctor-led practice has an obligation to put the patient’s clinical interests first.
Beyond safety screening, a doctor’s consultation plays a direct role in determining whether Pico laser is the right treatment for a given pigmentation concern — and if so, what the appropriate protocol looks like.
This is where the topic of melasma requires specific and honest discussion.
Melasma is a chronic, hormonally influenced pigmentation condition that is extremely common in Singapore — particularly among women — and is frequently undertreated or incorrectly treated in the aesthetic industry. It is characterised by diffuse, symmetrical brown or greyish patches, most commonly on the cheeks, forehead, upper lip, and chin.
Here is the clinical reality that many aesthetic practices do not communicate clearly: laser treatment is not the first-line treatment for melasma. In fact, in many melasma patients, aggressive laser treatment can worsen the condition by triggering post-inflammatory hyperpigmentation or stimulating rebound melanin production. Melasma is driven by internal factors — sun exposure, hormonal fluctuations, heat — that laser treatment does not address. Without managing these root causes, the pigmentation returns.
At VIDASKIN, our first-line treatment for melasma is Cosmelan or dermamelan — clinically validated, physician-applied depigmentation programmes that address both the visible pigmentation and the underlying melanogenesis pathway. These treatments produce measurable, lasting results in melasma patients when combined with appropriate sun protection and maintenance, and they do not carry the risk of laser-induced rebound that makes aggressive laser treatment problematic in this condition.
So why do so many aesthetic clinics in Singapore recommend laser as the go-to treatment when a melasma patient walks in? Candidly, because it is an easier sale. Patients often arrive expecting a laser. They have seen it advertised, they associate it with modern technology, and they are sometimes disappointed when a doctor tells them something different. Recommending a laser to a patient who expects a laser is commercially convenient. It is not always clinically correct.
At VIDASKIN, we make it our responsibility to educate our patients rather than to tell them what they want to hear. If you have been told by other providers that laser is the answer for your melasma, we would encourage you to come in for a consultation. We are happy to show you clinical before-and-after results from patients treated with cosmelan and dermamelan — and to have an honest conversation about what treatment approach is most likely to work for your specific pigmentation. Book a pigmentation consultation at VIDASKIN and let our doctors give you a diagnosis-first assessment.

What types of hyperpigmentation does Pico laser treat?
Pico laser is effective for a range of pigmentation conditions, including solar lentigines (sun spots), post-inflammatory hyperpigmentation (PIH), freckles, café-au-lait macules, and certain types of dermal pigmentation such as Hori’s naevus. The appropriate treatment approach depends on the type, depth, and underlying cause of the pigmentation, which can only be determined through a doctor’s assessment.
Is Pico laser safe for darker skin tones?
Yes — Pico laser is considered one of the safer laser options for darker skin phototypes (Fitzpatrick III to V), which are common in Singapore’s patient population. Its photoacoustic mechanism generates less heat than traditional nanosecond lasers, reducing the risk of post-inflammatory hyperpigmentation (PIH). However, correct parameter selection by an experienced doctor is essential — safety is not guaranteed by the technology alone.
Why does my pigmentation look darker after Pico laser?
Temporary darkening of treated lesions in the days following a Pico laser session is an expected response. The fragmented melanin particles are still present within the tissue and have not yet been cleared by the body’s lymphatic system. This darkening typically resolves over one to three weeks as the clearance process progresses. Patients should avoid picking or rubbing the treated area during this phase.
How many Pico laser sessions are needed for pigmentation?
The number of sessions depends on the type, depth, and severity of the pigmentation. Superficial lesions such as mild sun spots may respond in one to three sessions; deeper or more complex pigmentation may require four to eight sessions or more. Melasma is managed differently and is not typically a Pico laser indication at VIDASKIN — our doctors will advise on the most appropriate treatment programme during consultation.
Is Pico laser the right treatment for melasma?
At VIDASKIN, laser is not our first-line treatment for melasma. Melasma is a complex, hormonally influenced condition that is frequently worsened by aggressive laser treatment, which can trigger post-inflammatory hyperpigmentation and rebound melanin production. Our preferred first-line approach for melasma is cosmelan or dermamelan — clinically validated depigmentation programmes that address the underlying melanogenesis pathway. We encourage patients with melasma to book a consultation for an honest, diagnosis-led discussion before committing to any laser treatment.
Can Pico laser be used if I am not sure what type of pigmentation I have?
This is precisely why a medical consultation is the essential first step before any pigmentation treatment. Pigmented lesions vary significantly in their nature, depth, and clinical significance — some require cosmetic treatment, others require medical investigation. A doctor experienced in pigmentation will examine your skin, use dermoscopy where appropriate, and provide a diagnosis before recommending any treatment. Do not begin laser treatment for an undiagnosed lesion.
How long do Pico laser results for pigmentation last?
Results depend on the type of pigmentation and the underlying contributing factors. Sun spots treated with Pico laser can show lasting improvement, provided strict sun protection is maintained. Conditions with ongoing triggers — such as hormonal pigmentation or melasma — are more likely to recur if the root cause is not addressed. Your doctor will advise on maintenance treatment and lifestyle measures relevant to your specific pigmentation type.
Pico laser is a genuinely effective tool for the right types of hyperpigmentation — but it is not the right tool for every dark spot, and it should never be the starting point before a proper diagnosis has been made.
At VIDASKIN, we begin every pigmentation consultation with a clinical assessment — examining the lesion, determining its type and depth, ruling out any conditions that require medical rather than cosmetic management, and then recommending a treatment plan that is genuinely appropriate for what you have. If Pico laser is the right choice, we will tell you why, how many sessions to expect, and what the realistic outcome looks like. If it is not the right choice — as is often the case with melasma — we will explain why, and present you with the evidence-based alternatives that are more likely to deliver lasting results.
We are a doctor-owned and doctor-led practice. That means our recommendations are based on clinical evidence and your best interests — not on what is easiest to sell or what you arrived expecting to hear. If you have concerns about pigmentation and want an honest, diagnosis-first assessment, book a consultation at VIDASKIN. We are happy to walk you through our approach, share clinical results, and give you the information you need to make a genuinely informed decision.
